TL;DR
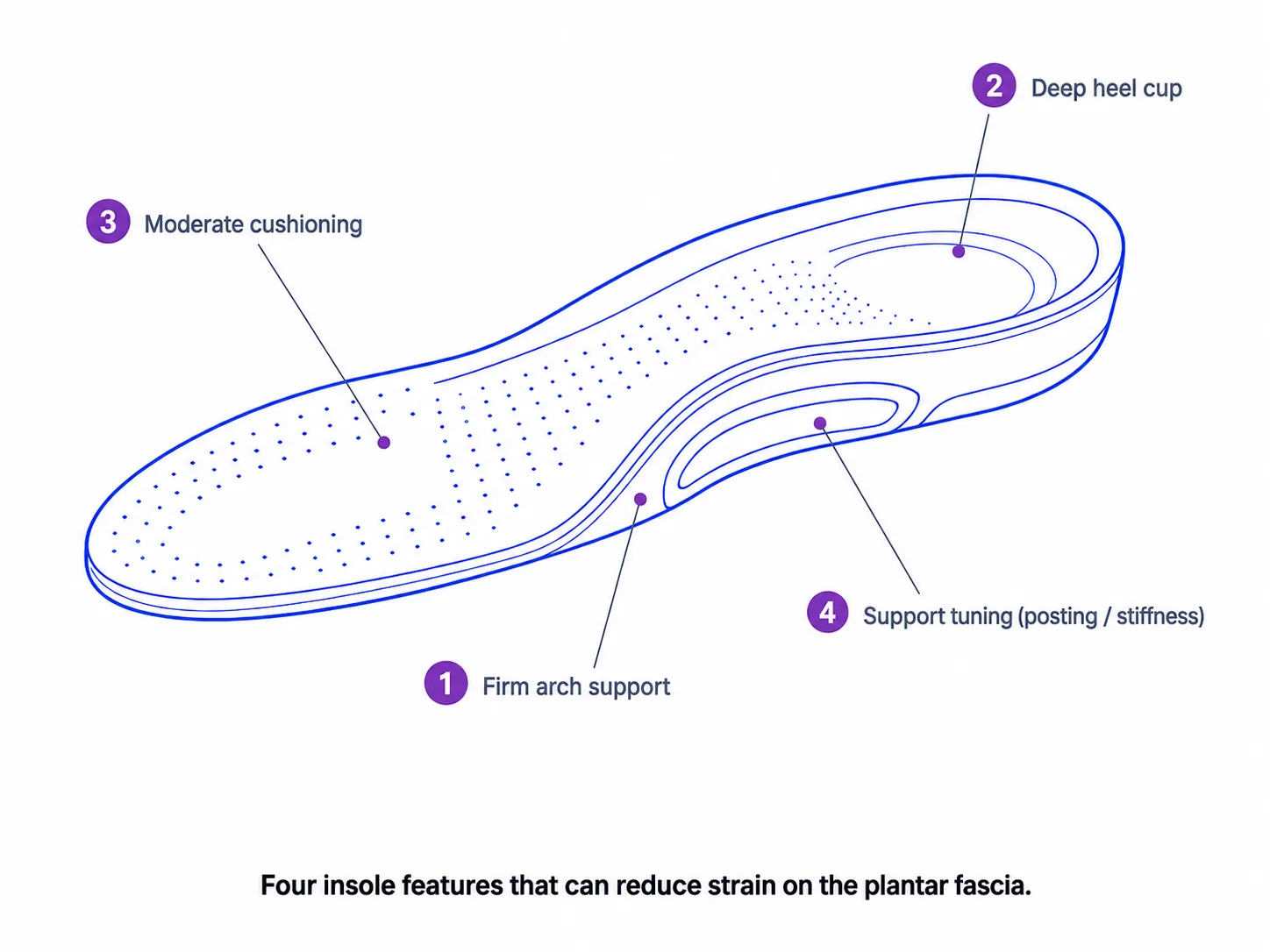
For plantar fasciitis-related heel discomfort, three insole design features tend to matter most: firm arch support matched to the wearer's arch height, a deep heel cup that helps stabilize the heel fat pad, and moderate cushioning with structure underneath rather than a soft insert. These may help distribute load and make standing and walking more tolerable, but response varies and insoles do not cure plantar fasciitis or replace clinical care.
Pre-made inserts suit mild cases; custom is worth considering for unusual arches, asymmetry, or high activity demands. Ergono3D sits on the custom 3D-printed insole side: guided inputs and parametric design generate a printable STL — a design tool, not a diagnosis or treatment, and not a substitute for clinical care.
Key takeaways
- Keep medical and product separate. Plantar fasciitis is a clinical category; insole shopping is a product one. This guide covers design choices, not diagnosis or treatment.
- Three features matter most. Firm arch support matched to arch height, a deep heel cup, and moderate cushioning with structure underneath — these may help redistribute load.
- Firm beats soft for many wearers. A very soft insert can let the arch flatten under load; structure first, cushioning second tends to hold the contour, though preference varies.
- Pre-made first, custom when it stops fitting. Templates suit mild cases; custom helps with unusual arches, left-right asymmetry, specific pressure points, or high activity demands.
- Iteration is the custom advantage. A parametric design can be revised — raise arch height, deepen the heel cup, change stiffness — instead of replacing a fixed insert.
- See a clinician when symptoms warrant it. Persistent, severe, bilateral, numb, tingling, or radiating heel pain needs evaluation. Ergono3D is a design tool, not a diagnosis, treatment, or substitute for clinical care.
People searching for insoles for plantar fasciitis usually are not looking for a generic anatomy lesson. They have heel pain, they want to know which insole features matter, and they need a practical way to choose between pre-made inserts and custom insoles. The hard part is that plantar fasciitis sits in a medical category, while insole shopping sits in a product category. Good advice has to keep both sides clearly separate.
Medical disclaimer
This article is educational and is not medical advice. It does not diagnose plantar fasciitis, prescribe care, or replace a podiatrist, physician, physiotherapist, or other licensed clinician. Insoles can be part of supportive foot-care management, but they are not a standalone treatment, a diagnostic tool, or a substitute for professional evaluation. Persistent or severe heel pain should be evaluated by a clinician.
Ergono3D's role is squarely on the product-design side: arch height, heel cup depth, TPU stiffness, posting, and iteration. This guide explains how those insole design choices relate to plantar fascia load and heel comfort. It does not diagnose the cause of heel pain and does not promise a clinical outcome.
What plantar fasciitis is, in one careful paragraph.
Plantar fasciitis is one of the most common sources of heel pain — but heel pain is not always plantar fasciitis. That distinction matters before any product choice.
Mayo Clinic describes plantar fasciitis as inflammation of the thick band of tissue that runs across the bottom of the foot and connects the heel bone to the toes. The classic symptom is stabbing pain near the heel, often worst with the first steps after waking or after long sitting. Flat feet, high arches, prolonged standing, running, and excess body weight can all affect how load reaches the plantar fascia.
AAOS adds an important point: heel spurs and plantar fasciitis are often discussed together, but they are not the same thing. A heel spur can show on imaging without being the cause of pain. For an insole buyer, the safer goal is not to self-diagnose from a symptom label, but to understand how supportive footwear and insole geometry may change pressure and strain while the underlying issue is being evaluated or managed.
Where Ergono3D fits — and where it does not.
Ergono3D is a custom insole design workflow. It is not a diagnosis tool, not a treatment, and not a podiatrist replacement.
For plantar fasciitis-related discomfort, Ergono3D should be understood as a product-design workflow, not a diagnosis or treatment tool. It helps users create and refine supportive insole geometry — arch height, heel cup depth, stiffness, and TPU structure — while clinical care remains the right path for persistent, severe, or complex heel pain.
Practically, this means Ergono3D sits on the custom side of the buying decision: a guided survey collects foot inputs, parametric design generates a print-ready STL, and TPU 3D printing produces a wearable insole that can be revised after real use. Compared with traditional clinical custom orthotics, the workflow is usually cheaper, faster, and easier to iterate on. It does not replace the clinical assessment, imaging, taping, splinting, or therapy that some heel pain cases need.
Why heel pain happens and where insoles fit in.
Heel pain insoles are adjunct supportive products. They change load and contact under the foot, but they do not resolve every source of heel pain.
AAFP describes plantar fasciitis as a common cause of adult heel pain and lists prolonged standing, excessive running, excessive pronation, and obesity as risk factors. Mayo's care guidance notes that clinicians may recommend off-the-shelf or custom-fitted arch supports to help distribute pressure more evenly. That is the key insole mechanism: not magic cushioning, but force distribution.
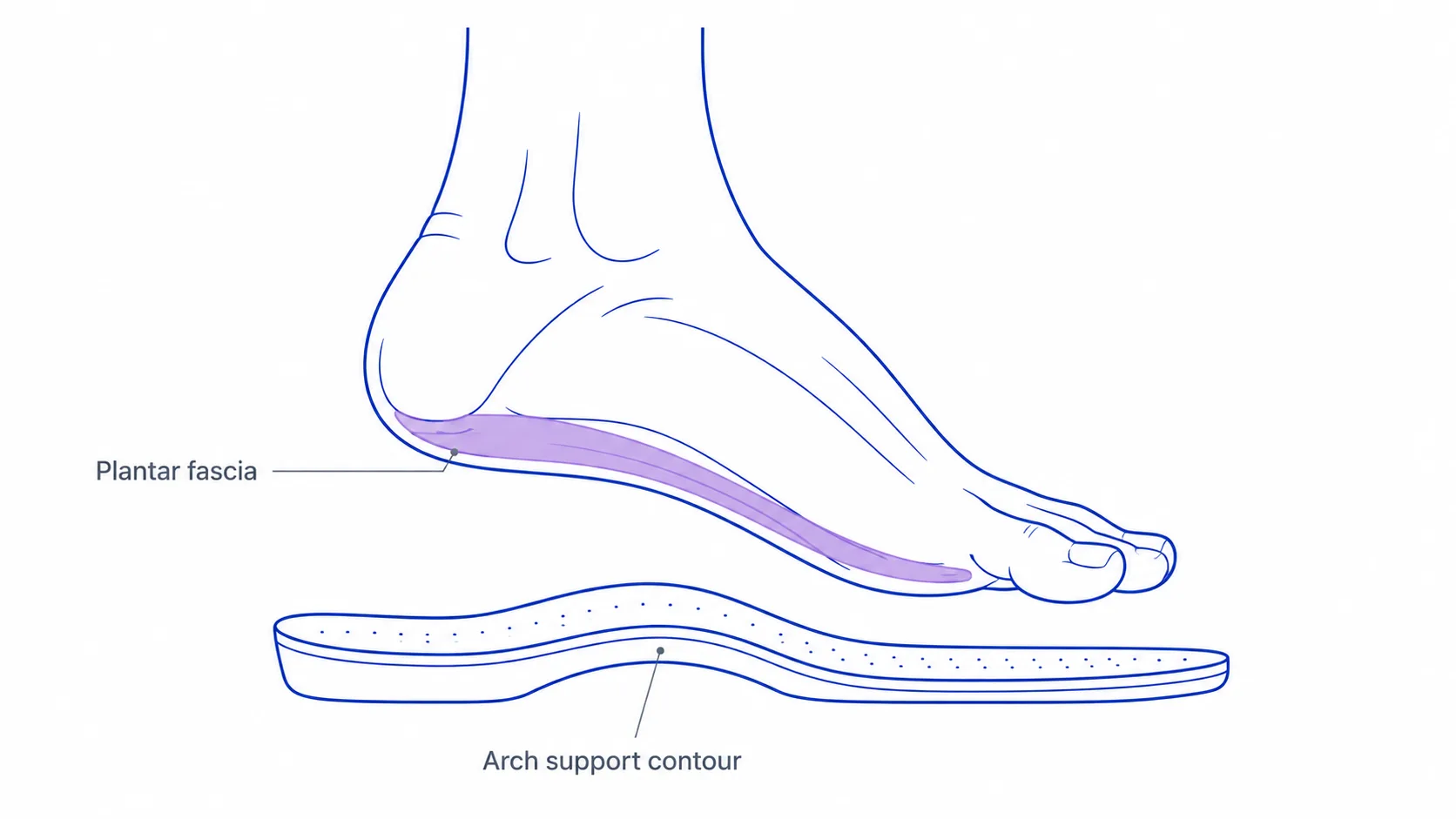
The plantar fascia helps support the medial longitudinal arch and absorbs shock during the gait cycle. When the arch drops too much under load, the fascia can stay under tension. When the heel is unstable inside the shoe, the heel fat pad and rearfoot can shift, which some wearers find increases local discomfort. When the insert is too soft, the wearer may sink into the cushioning while the arch continues to flatten. A well-designed plantar fasciitis insole tries to manage these three things at once: arch support, heel containment, and controlled cushioning.
For a deeper look at foot-to-insole mechanics, see our science behind custom insoles. The short version is that the insole is an interface. It cannot change the diagnosis, but it can change how the foot meets the shoe during standing, walking, and sport.
Insole design features that matter for plantar fasciitis.
The best-fitting insoles for plantar fasciitis are usually not the softest. The more important question is whether the support holds the arch and heel in a useful shape under real load.
1. Firm arch support matched to arch height
Useful arch support meets the wearer's arch without acting like a hard ridge. If the contour is too low, the arch may continue to flatten under body weight. If it is too high or positioned too far back, it can create a new pressure point. The aim is firm, shaped support that matches the wearer's arch height and arch length. Generic "high support" is not the same as good support — useful arch support for plantar fasciitis should share load, not introduce a new sore spot.
2. Deep heel cup
A deeper heel cup cradles the calcaneus and reduces side-to-side movement inside the shoe. The heel fat pad is part of the foot's natural shock-absorbing system, and a heel cup can help keep that pad centered under the heel during stance. It also gives the insole a more stable rearfoot base, which matters when discomfort changes how the wearer loads the foot.
3. Moderate cushioning, with structure underneath
Cushioning still matters. A hard plastic shell with no top layer can be uncomfortable for sensitive heels. The common pitfall is assuming softer is always better. For many people, moderate cushioning that absorbs surface pressure while the arch structure underneath holds its shape works better than a very soft insert that collapses under load, leaving the foot padded but unsupported. Individual preference and clinical context vary.
4. Full-length versus three-quarter length
Full-length insoles cover heel, arch, and forefoot. They usually feel more stable in athletic shoes or work shoes because they do not end abruptly under the metatarsal area. Three-quarter inserts can work in tighter dress shoes, but they may shift and feel less integrated. For plantar fasciitis discomfort, full-length is usually the safer first option unless shoe space is limited.
5. TPU material response and print structure
When the insole is 3D printed in TPU, hardness (often expressed in Shore A) and internal infill structure together determine how the insole feels under load. A heavier wearer or someone standing all day may need a firmer TPU and denser support zones than a lighter, casual user. For a practical map of the adjustable controls, read our parameters guide.
A practical fit check after a few minutes of wear: the arch should feel contacted, not jabbed; the heel should feel centered, not squeezed; the forefoot should sit flat enough that the shoe still bends naturally. If a hard ridge appears under the medial arch within minutes, the arch height may be too high or too far back. If the heel still slides, heel cup depth is probably too shallow or the shoe has too much internal volume. If the insert feels soft but the arch still drops, the material is cushioning the surface without supporting the structure.
Soft vs firm: the most common mistake.
Heel pain makes people reach for softness. Plantar fascia strain often needs structure first and cushioning second.
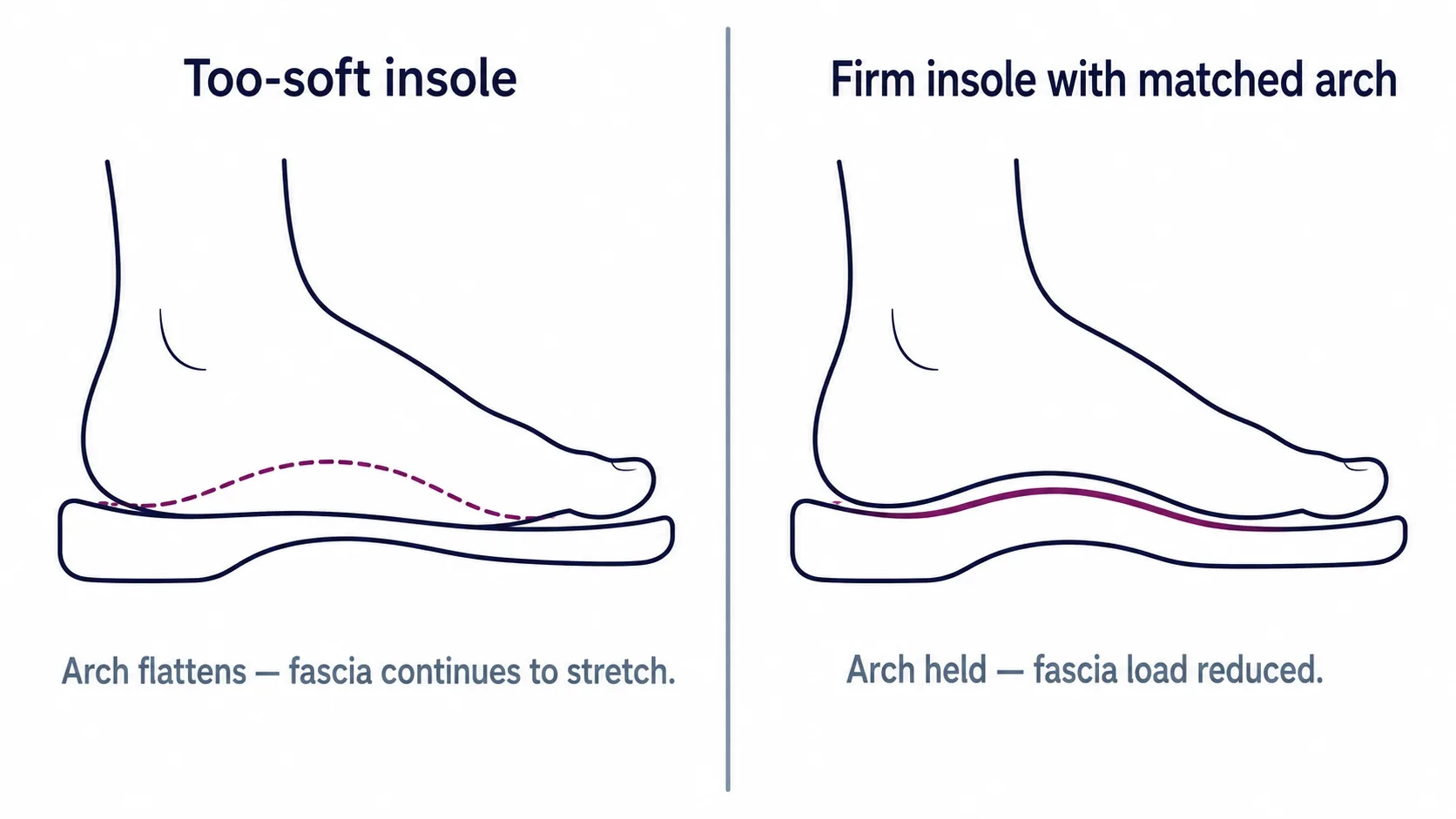
The instinct is understandable: the heel hurts, so the insole should be soft. Very soft heel pads can feel better for the first few minutes, but they may not change the arch mechanics that keep the fascia under stretch. A too-soft insole compresses under body weight. If the arch area collapses with it, the fascia can continue to experience tension even though the heel feels padded.
Firm does not mean harsh. The useful combination is firm structure under the arch, a stable heel cup, and a moderate top layer. That gives the wearer contact area, shape, and some cushioning without turning the insert into a sponge. It is the design logic behind most well-regarded plantar fasciitis insoles: a contoured, semi-rigid support with enough surface comfort to be worn consistently.
Exact firmness still depends on the wearer. A high-arch foot may need more contact and cushioning. A low-arch foot may need firmer support that resists collapse. A heavier user or someone standing all day may need a firmer TPU or denser print structure than a lighter wearer using the insole casually.
Pre-made vs custom for plantar fasciitis.
Custom insoles for plantar fasciitis make the most sense when standard shapes keep missing the wearer's foot, or when the wearer needs different geometry on each side.
Pre-made insoles — brands such as Superfeet, Powerstep, and Dr. Scholl's — are a reasonable first step for many people. They are available immediately, cost less, and often include a firmer arch than the removable sockliner that shipped with the shoe. They are especially reasonable when symptoms are mild, the wearer has a roughly neutral arch, and no previous insole has been tried. They are a useful first option for many people with mild, non-complex heel discomfort and should not be dismissed.
The structural limit of pre-made insoles is that they are templates. The wearer picks the closest match from a small set of arch heights, lengths, and heel cup shapes. There is no way to fine-tune arch height, heel cup depth, stiffness, or TPU material response per left and right foot. There is no way to iterate after wearing the insole in real shoes for a few weeks. For most people, that ceiling is acceptable. For people with significant asymmetry, unusual arch height, specific pressure points, or high activity demands, it is the point at which the pre-made path runs out.
Custom takes two main forms. Traditional clinical custom orthotics — a podiatrist or orthotics lab takes a cast or scan, prescribes the geometry, and a lab fabricates the device. This is the right path for complex cases, high-risk conditions such as diabetic neuropathy, or when a clinician has already identified specific corrective needs. Ergono3D's parametric workflow — a guided survey collects the relevant foot inputs, parametric design generates an STL, and TPU 3D printing produces the insole. The wearer can revise arch height, heel cup depth, posting, and stiffness, then reprint without restarting the whole process.
Both are custom. The difference is cost and iteration speed: Ergono3D is generally cheaper and faster to revise than a lab orthotic, which is what makes the iteration loop practical. Clinical custom orthotics remain the right choice when a clinician is actively managing the case or when prescription-level intervention is needed.
That iteration loop matters because plantar fasciitis-related discomfort is not static. A wearer may tolerate more arch contact after a few weeks of supportive footwear, or may find that one foot needs a different medial contour than the other. With a fixed retail insert, the only adjustment is replacing the product. With a parametric design, the adjustment can be smaller: raise arch height 1–2 mm, increase rearfoot stiffness, deepen the heel cup, or switch from a softer TPU setting to a firmer one. The goal is not to self-manage a medical condition in isolation. The goal is to avoid defining "custom" as a one-shot guess when the product fit can be refined.
For more on the custom side specifically, see custom arch support insoles and are custom insoles worth it?. For the manufacturing background, see how insole manufacturing is evolving.
Activity-specific considerations.
Insoles for standing all day and insoles for running often need different priorities, even when the underlying discomfort is similar.
Standing all day
Long standing loads the heel and arch for hours with little recovery. The important features are a stable heel cup, a firm but wearable arch contour, and enough top-layer cushioning to reduce surface irritation. Work boots may also need more volume control because thick socks, steel toes, and rigid midsoles change how much space the insole has.
Running
Running increases impact and repetition. The insole should not be so soft that the foot sinks and rolls unpredictably. A firm arch, stable rearfoot, and smooth transition toward the forefoot tend to matter more than a thick pad. Runners should be especially cautious with sharp or worsening heel pain and should reduce load if symptoms escalate, then talk to a clinician.
Court sports
Court sports add lateral cuts and quick stops. The insole still needs arch and heel support, but the shoe-insole combination also needs side-to-side stability. A tall, soft insert in a court shoe can feel unstable. A lower-profile, firmer design often works better when the shoe already provides strong cushioning.
When to see a clinician.
This is the most important section in the article. Product experimentation should stop when symptoms suggest a clinical evaluation is needed.
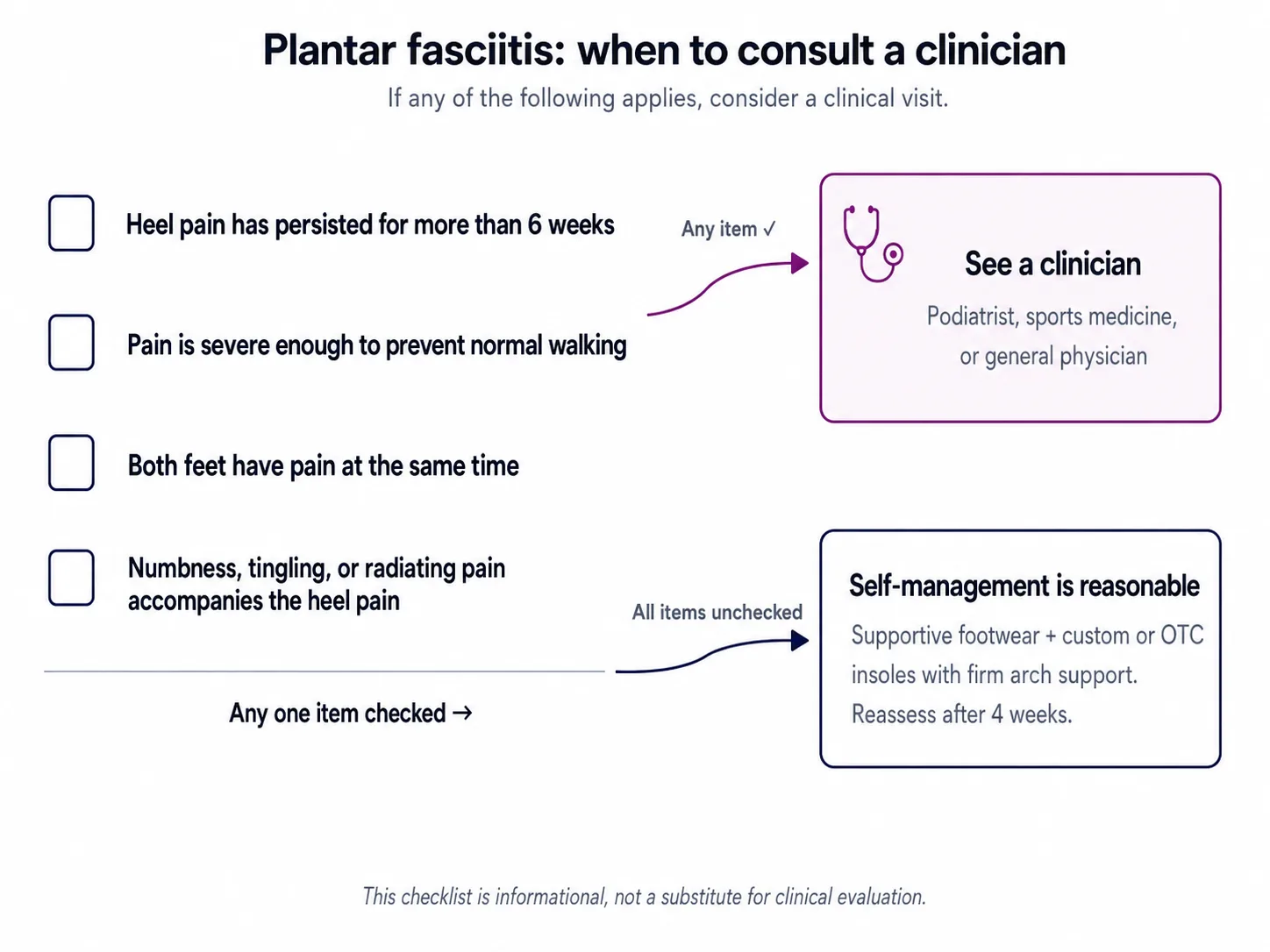
A mild heel ache that improves with rest, supportive footwear, and lower activity load is different from persistent or disabling pain. As a practical threshold, a clinical visit is more appropriate than continued insole experimentation when any of the following are present:
- Heel pain that has lasted more than 6 weeks despite supportive footwear and activity changes
- Pain severe enough to prevent normal walking, or inability to bear weight
- Recent trauma, fall, or acute injury to the foot or ankle
- Visible swelling, redness, warmth, bruising, or deformity
- Fever accompanying the pain
- Numbness, tingling, burning, or pain that radiates up the leg
- Bilateral heel pain that appears suddenly and strongly
- Rapidly worsening pain, or pain that wakes the wearer at night
- Diabetes, peripheral neuropathy, poor circulation, or other conditions that raise foot-health risk
- Recent foot or ankle surgery, or any active medical management of the foot
The right clinician may be a podiatrist, sports medicine physician, physiotherapist, or general physician, depending on location and access. A clinician can confirm whether the pain pattern actually fits plantar fasciitis, rule out other heel problems such as stress fracture or nerve involvement, and decide whether imaging, physical therapy, taping, night splints, medication, injections, or other care is appropriate.
APMA's heel pain resources note the overlap between plantar fasciitis and heel spur presentations, while Mayo and AAOS both stress that symptoms and diagnosis should be interpreted clinically. That is why Ergono3D frames insoles as supportive design products. They can be useful, but they should not delay clinical care when the pattern is outside a low-risk comfort problem.
Not medical advice
This checklist is informational. It is not a diagnosis, triage service, or substitute for professional evaluation. If symptoms are persistent, severe, changing, bilateral, numb, tingling, or radiating, consult a clinician.
Use Ergono3D to design a custom insole — guided inputs, parametric arch support and heel cup depth, TPU stiffness options, print-ready STL. Free preview, 5 credits, no card required.
Ergono3D is a custom insole design workflow, not a diagnosis or treatment tool. For persistent, severe, or complex heel pain, please see a clinician.
FAQs about insoles for plantar fasciitis.
What insole features matter for plantar fasciitis discomfort?
Three features tend to matter most for many people: structured arch support matched to the wearer's arch height, a deep heel cup that helps stabilize the heel fat pad, and moderate cushioning that does not collapse under load. Insoles with these features may reduce strain on the plantar fascia during weight-bearing activity, but individual response varies and insoles are not a standalone treatment or a substitute for clinical care.
Can insoles cure plantar fasciitis?
No. Insoles support the foot and can redistribute load, which some people find makes standing and walking more tolerable, but they do not directly resolve the underlying tissue irritation, overuse pattern, or medical cause of heel pain. Conservative management usually involves a combination of supportive footwear, activity changes, stretching, and clinical care when symptoms persist.
Should plantar fasciitis insoles be soft or firm?
For many people, a structured, contoured arch support with a moderate top layer is more useful than a very soft insert that collapses under load and lets the arch flatten. Individual preference and clinical context vary; some wearers may prefer a softer setup, especially when heel fat-pad sensitivity is the dominant issue.
How long does it take to know whether an insole is helping?
Some wearers notice reduced first-step discomfort within days. Others need 2–4 weeks of consistent wear to feel a meaningful difference. If symptoms have not improved after 4–6 weeks of supportive insoles and footwear changes, it is worth consulting a clinician.
Pre-made or custom — which should I try first?
Pre-made insoles with structured arch support may be a reasonable first step for many people with mild, non-complex heel discomfort. Custom becomes worth considering when arches are unusually high or low, when there is significant left-right asymmetry, when activity demands are high, or when several pre-made options have already failed to provide a good fit. Persistent, severe, or atypical pain should be evaluated by a clinician regardless of insole choice.
Are 3D printed custom insoles an option for plantar fasciitis?
They can be an option on the product-design side when the goal is a more adjustable insole shape: arch height, heel cup depth, posting, stiffness, and left-right differences can be tuned and reprinted. A 3D printed custom insole is not a treatment or diagnosis for plantar fasciitis, and persistent or severe heel pain should be assessed by a clinician.
How does Ergono3D fit into custom insole design for plantar fasciitis?
Ergono3D is a custom insole design workflow, not a diagnosis or treatment tool. It uses guided inputs and parametric design to generate a print-ready STL for TPU 3D printing, with adjustable arch height, heel cup depth, posting, and stiffness per foot. It sits on the custom side of the decision — generally cheaper, faster, and more iterable than traditional clinical custom orthotics — but it does not replace clinical care for persistent or complex heel pain.
When should I see a clinician about plantar fasciitis?
Heel pain lasting more than 6 weeks, pain severe enough to prevent normal walking, pain in both feet at the same time, or pain accompanied by numbness, tingling, or radiating sensations should be evaluated by a podiatrist, sports medicine physician, physiotherapist, or general physician. Insoles are an adjunct, not a substitute for clinical care.
More: custom insoles vs foam inserts · making your own custom insoles at home · why custom insoles matter.